


COVID-19 Mortality Working Group: Almost 20,000 excess deaths for 2022 in Australia
Catch up on the Actuaries Institute’s COVID-19 Mortality Working Group’s latest analysis of excess deaths.
In summary:
|
Background
The COVID-19 Mortality Working Group has examined the latest Provisional Mortality Statistics, covering deaths occurring prior to 30 November 2022 and registered by 31 January 2023, released by the Australian Bureau of Statistics (ABS) on 24 February.
This release also included the article COVID-19 Mortality in Australia, with details on all COVID-19 deaths occurring and registered by 31 January 2022.
This is our first detailed analysis since the 31 August data was released. Therefore, much of our commentary focuses on the three months to 30 November 2022. We also provide an indicative estimate of excess mortality for the month of December 2022.
Consistent with the terminology used by the ABS and reflective of the data provided, throughout this article, we separate COVID-19 deaths into:
- deaths “from COVID-19”, namely deaths where COVID-19 is listed as the primary/underlying cause of death; and
- deaths “with COVID-19”, namely deaths where the underlying cause of death has been determined as something other than COVID-19, but COVID-19 was a contributing factor mentioned on the death certificate.
In this article, we calculate excess deaths by comparing observed deaths to our “baseline” predicted number of deaths for doctor-certified deaths (by cause) and coroner-referred deaths (for all causes combined).
The Working Group has also examined excess mortality by age/gender and by state/territory. In so doing, we have used additional data supplied by the ABS in a customised report in relation to COVID-19 deaths registered by 31 January 2023, namely:
- the number of deaths each week both from COVID-19 and with COVID-19, broken down by age/gender; and
- the number of deaths each week both from COVID-19 and with COVID-19 for each of NSW, VIC and QLD, plus deaths from COVID-19 for WA and SA. Due to small numbers, the ABS is unable to supply weekly COVID-19 deaths for the smaller states/territories.
Baseline Predictions
Our previous Actuaries Digital article discussed in some detail how we arrived at our baseline predicted deaths. In short:
- Our baselines by cause of death are set by extrapolating linear regression models fitted to Standardised Death Rates (SDRs), which are then re-expressed as numbers of deaths.
- For our baselines by age/gender and by state/territory, we have used a slightly different, and more approximate, approach because SDRs are not available.
- Given the slight difference in approach, we end up with small differences in the total predicted numbers of deaths from our cause, age/gender and state/territory models, with increasing deviation as the projection period extends.
- Our models by cause of death remain the base for our “best estimate” of total excess mortality, as we believe that they best reflect the underlying mortality trends in Australia.
The baselines for our estimates of excess deaths remain “in the absence of the pandemic” for each of the three years 2020 to 2022. We have not included any COVID-19 deaths in the baseline, as these would not exist in the absence of the pandemic.
As always, it is important to note that predicted death numbers are increasing faster from demographic changes (ageing and population size) than they are reducing due to mortality improvement. Therefore, our model predicts higher baseline numbers of deaths in each successive year.
Comparison with ABS reporting
The results we present here differ from those quoted by the ABS in its commentary surrounding the release of the Provisional Mortality Statistics. The ABS explicitly states that the comparison presented is not an official estimate of excess mortality and that their baseline for 2022 (being the simple average of the number of deaths from 2017, 2018, 2019 and 2021, with no allowance for mortality trends or demographic changes) serves as a proxy for the expected number of deaths only.
For example, the latest Provisional Mortality Statistics says: “In 2022, there were 174,717 deaths that occurred by 30 November and were registered by 31 January 2023, which is 22,886 (15.1%) more than the historical average.” By comparison, we estimate that there were 17,900 (11.3%) excess deaths in this period. The main reason for the difference between the ABS figure of 22,886 and our estimate of excess deaths of 17,900 is the difference in the baselines used.
Excess deaths to 30 November 2022
Figure 1 shows the results of our analysis, comparing actual deaths each week to our predicted values and the 95% prediction interval.
Figure 1 – Weekly actual and predicted deaths – All Causes
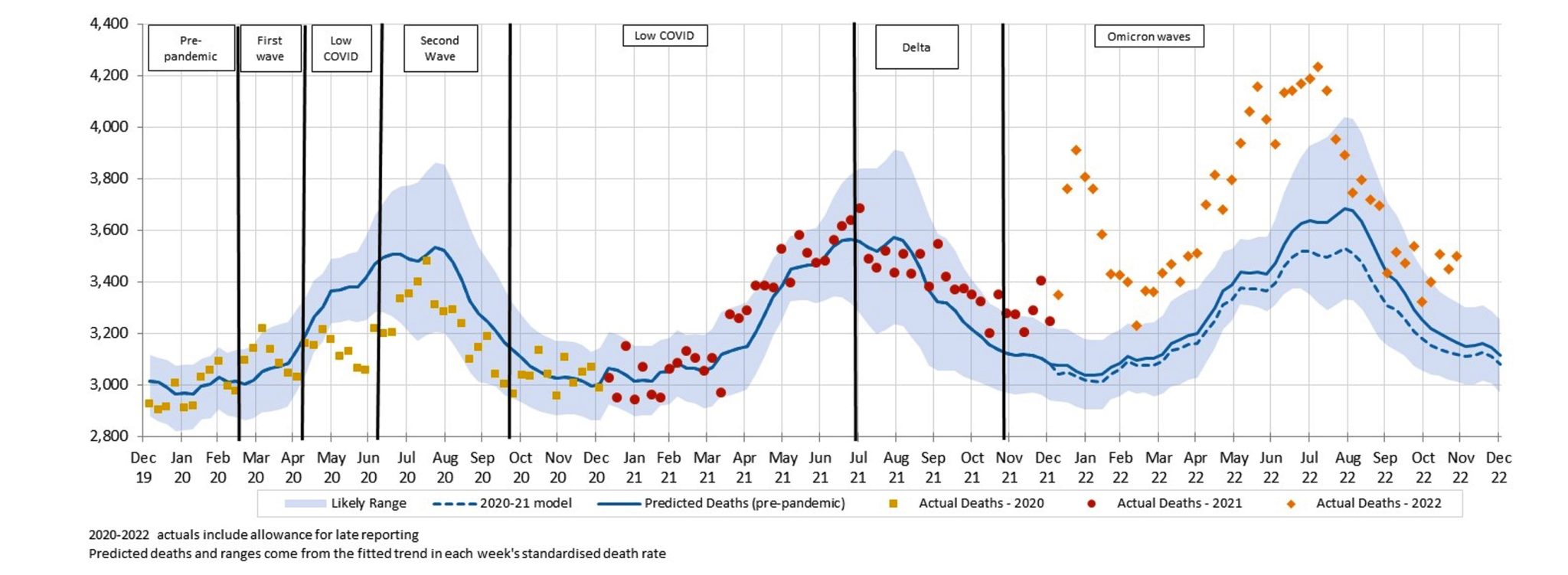
Deaths in September and October, while higher than the predicted level, were within the 95% prediction interval for all but one week. This is in stark contrast to earlier in the year when almost every week was well above the prediction interval (i.e. above the 97.5thpercentile). In November, however, the last three weeks were again well above the upper end of the prediction interval.
Figure 2 shows deaths from COVID-19 and with COVID-19, noting that, given small numbers, weekly data for with COVID-19 deaths is only available for 2022.
Figure 2 – Weekly actual deaths – Deaths from and with COVID-19*
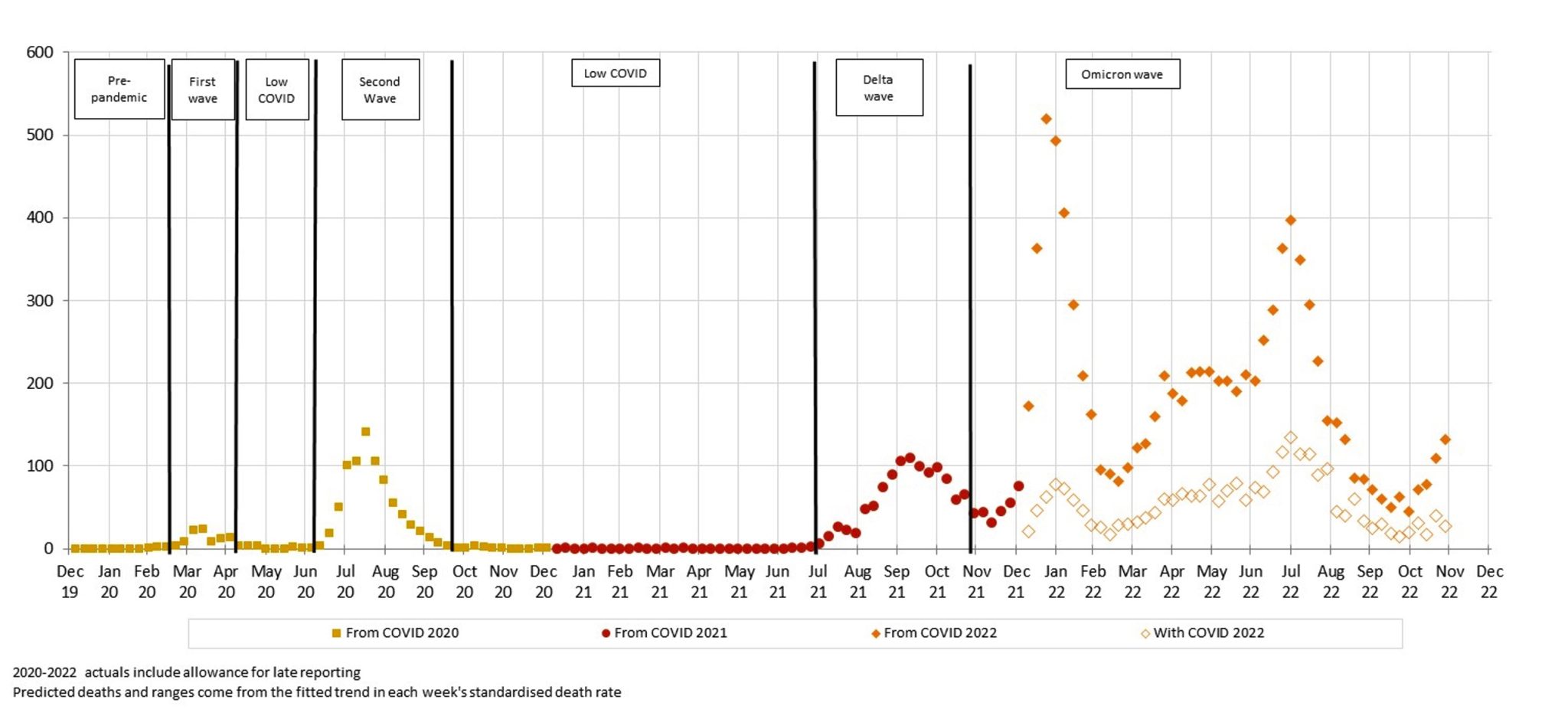
* COVID-19 data from ABS customised report 2023
Deaths from COVID-19 peaked in the last week of July, trended downwards until the end of October, and then rose again throughout November. Deaths with COVID-19 have followed the same pattern, although with a little more volatility given the smaller numbers of such deaths.
It is unclear how many people who died with COVID-19 would have died during this period anyway, and how many may have had their death hastened by COVID-19. However, given that with COVID-19 deaths follow the same peaks and troughs as from COVID-19 deaths, and that with COVID-19 deaths are only counted as such if COVID-19 is considered to have contributed to death, it seems that COVID-19 is a catalyst for with COVID-19 deaths, rather than being merely coincidental. We note that the same traditionally happens with the winter peak of respiratory disease deaths.
There may be instances where it is difficult to determine whether a death is due to COVID-19 versus COVID-19 being a contributing cause, and an element of professional judgment by the certifier will necessarily need to be exercised. It is unclear to us how often such decisions may need to be made, and how much “blurring” there may be between from COVID-19 and with COVID-19 deaths.
Figure 3 shows the comparison of actual deaths to predicted after removing from and with COVID-19 deaths.
Figure 3 – Weekly actual and predicted deaths – All Causes excluding deaths From and With COVID-19
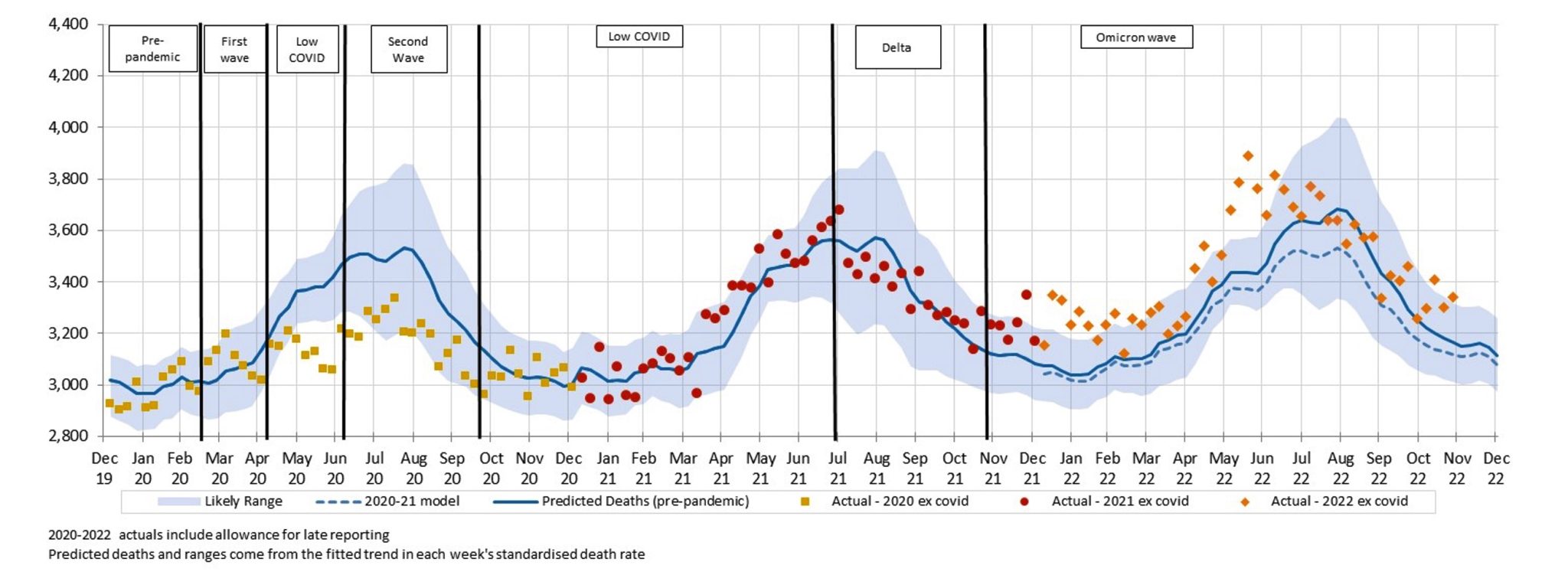
Even after removing all from and with COVID-19 deaths, significant excess mortality remains for 2022, with:
- A spike around the time of the January peak in COVID-19 deaths;
- another spike coinciding with the peak of the flu season (which this year came just before another peak of COVID-19 deaths) in late June; and
- indications of another spike in November when COVID-19 deaths were again on the increase.
Figure 4 – Weekly excess deaths – All Causes*

* COVID-19 data from ABS customised report 2023
This can be seen clearly in Figure 4, where we divide excess deaths into those from COVID-19, those with COVID-19 and the residual excess from other causes, set against the 95% prediction interval. The correlation of the trend of non-COVID-19 excess deaths with COVID-19 deaths can be seen in the 9-week centred rolling average. The next section discusses the causes of death driving this trend.
Excess deaths to 30 November 2022 by Cause of Death
Table 1 shows our estimate of excess deaths broken down by cause.
As in our previous work, we have assumed that coroner-referred COVID-19 deaths will be 5% of all COVID-19 deaths in 2022, based on the experience of late 2021 and the emerging experience in 2022. If our estimate of coroner-referred COVID-19 deaths is too high (or low), this will not affect the total level of excess deaths measured; it will just mean that our estimate of non-COVID-19 coroner-referred deaths will be too low (or high) by the same amount.
Table 1 – Excess deaths in Australia – By Cause of Death
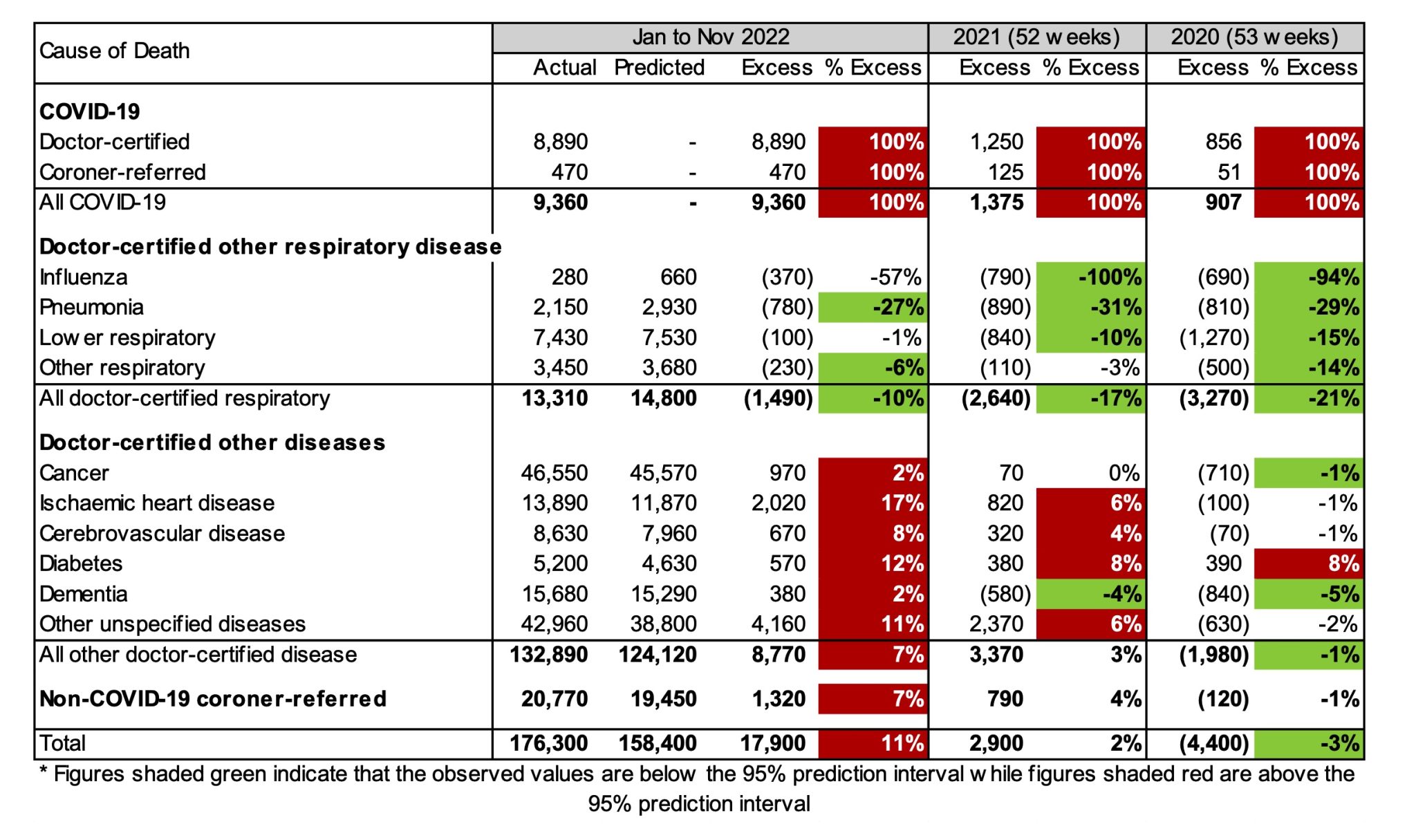
For the first eleven months of 2022:
- Total deaths were 11% (or +17,900) higher than predicted, compared with excess deaths of -4,400 for 2020 and +2,900 for 2021;
- there were 9,360 deaths from COVID-19, representing 52% of the excess deaths and including 167 deaths reported as due to Long Covid;
- while not shown in the table, 2,592 deaths with COVID-19 are included among the other causes of death, representing a further 14% of the excess deaths and meaning that 33% of excess deaths (c. 6,000) have no mention of COVID-19 on the death certificate;
- despite influenza circulating in Australia again in 2022, doctor-certified deaths from respiratory disease continue to be lower than expected (10% lower) although not as low as we saw earlier in the pandemic;
- while doctor-certified deaths from cancer and dementia are close to expected in percentage terms (both 2% higher), these differences are statistically significant;
- doctor-certified deaths from heart disease, cerebrovascular disease and diabetes were all significantly higher than predicted (by between 8% and 17%);
- doctor-certified deaths from other unspecified diseases were also significantly higher than predicted (by 11%), continuing a trend observed since April 2021. Note that this is a large “catch-all” category and it is difficult to infer the reason for this large increase, although history suggests that non-ischaemic heart diseases probably make up more than 25% of deaths from other unspecified causes; and
- non-COVID-19 coroner-referred deaths were 7% higher than expected.
Figure 5 and Figure 6 show weekly excess deaths by underlying cause (thus including deaths with COVID-19) since the start of the pandemic, compared with the 95% prediction interval. All graphs are shown using the same y-axis to give a sense of the contribution of each cause. The 9-week centred average is also shown, to highlight any trends.
Figure 5 – Weekly excess deaths in 2020-22 for cancer, heart, stroke, and diabetes
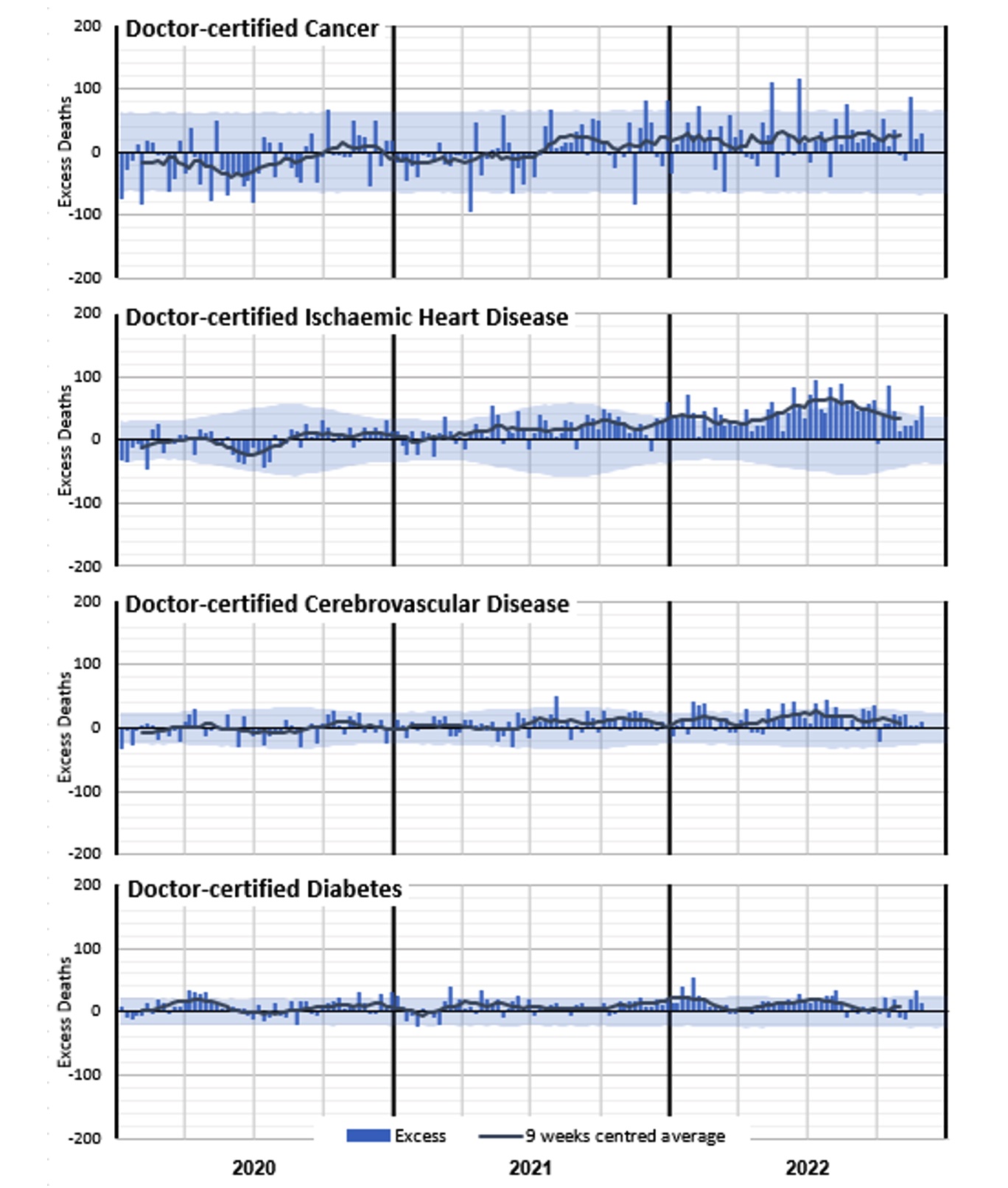
Figure 5 shows a clear increase in excess deaths due to ischaemic heart disease from around March 2021 until around August 2022, with the peaks and troughs following the same timing as deaths from COVID-19 (noting that each chart includes deaths from that cause with COVID-19). There has been a consistent, albeit volatile, excess for deaths from both cancer and cerebrovascular disease since around July 2021. Diabetes deaths have generally been higher than expected throughout the pandemic, and again the peaks and troughs have followed the same patterns as deaths from COVID-19.
Of these causes, ischaemic heart disease is the biggest contributor to excess deaths in 2022, followed by cancer.
Figure 6 – Weekly excess deaths in 2020-22 for other causes
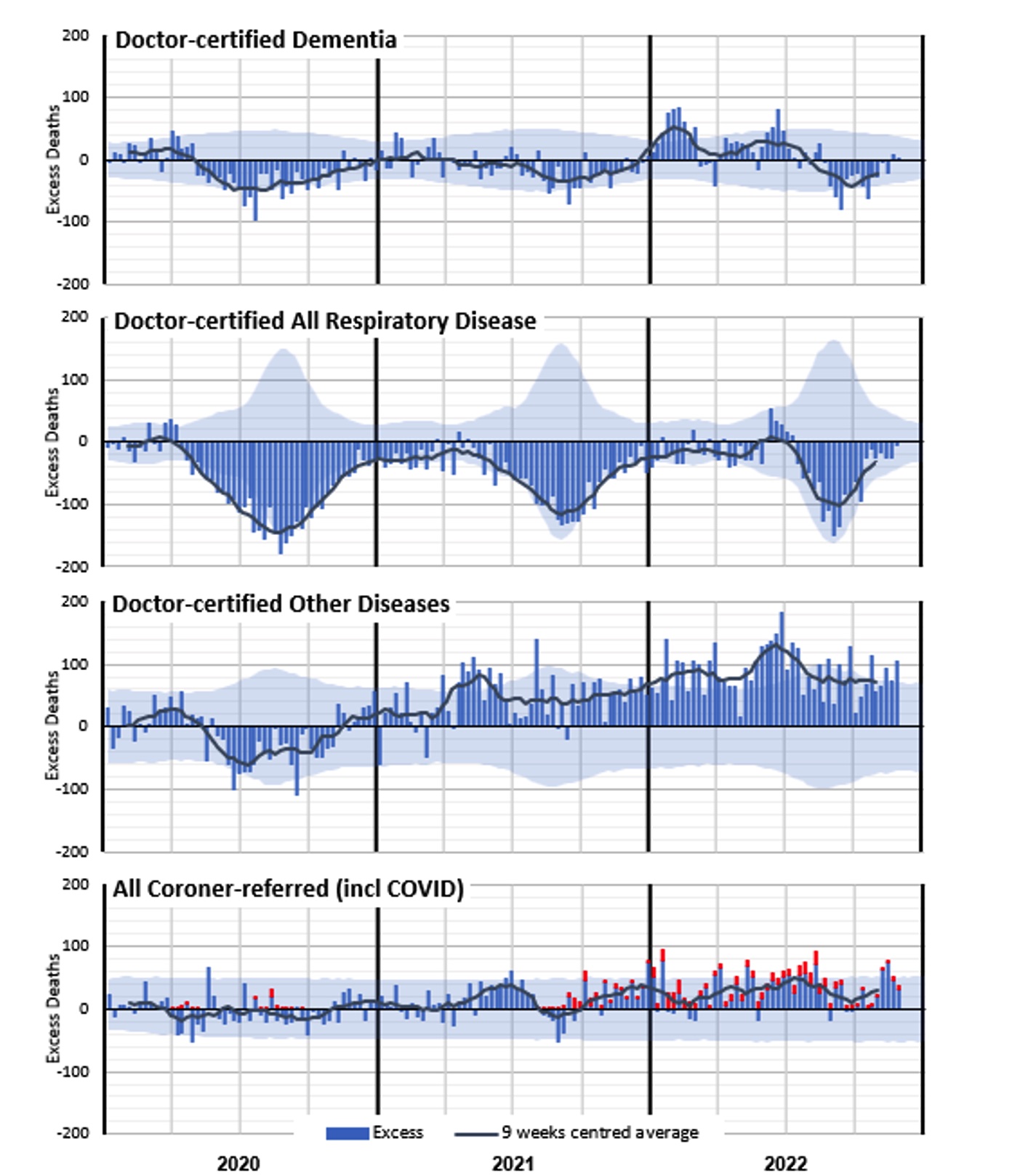
Figure 6 shows negative excess deaths for dementia in 2020, 2021 and September/October 2022 (closely correlated with lower respiratory disease), with higher excess deaths in the first half of 2022 (closely correlated with COVID-19 and flu waves). Deaths from respiratory disease have been significantly lower than expected throughout the pandemic, except for the short (and early) flu season which peaked in late June 2022. This coincides with the second 2022 peak in excess non-COVID-19 deaths that we saw in Figure 3and Figure 4.
Deaths from other diseases (where available ABS data does not specify the cause) were also lower than predicted in 2020 (correlated with lower respiratory disease) but have been, as a group, the largest contributor to non-COVID-19 excess deaths in 2021 and 2022. It is not clear what might be driving this, although we expect that at least part of the excess will be in respect of people who otherwise may have succumbed to respiratory disease in 2020 and 2021. We also note that deaths from heart conditions other than ischaemic heart disease traditionally comprise more than 25% of this group and that there does appear to be an increased risk of heart disease after recovering from COVID-19.
Coroner-referred deaths include deaths from COVID-19. In Figure 6, we have separately shown these (in red), using actual coroner-referred COVID-19 deaths for 2020 and 2021, and estimates for 2022 based on our assumption that 5% of all COVID-19 deaths are referred to the coroner. The residual non-COVID-19 coroner-referred deaths are well above expected levels in the second half of 2021 and throughout 2022. We note, however, that suicide monitoring reports for NSW and Victoria show a slight increase in 2022, but not large enough to account for the level of excess seen in those states. Similarly, Australia-wide road death statistics show a small increase in 2022, but not large enough to account for the overall increase.
Excess deaths for the full year 2022
While the ABS Provisional Mortality Statistics data is only available up to the end of November 2022, we have formed an estimate of excess deaths in the month of December 2022 to arrive at a full-year estimate for 2022.
We have:
- taken deaths both from and with COVID-19 in the month of December 2022 from the COVID-19 Mortality in Australia article, making allowance for late-registered deaths;
- assumed that any contribution to excess mortality from respiratory disease will be negligible in the month of December, which is a summer month; and
- assumed that excess mortality from other causes of death would be the same as in the month of November 2022, i.e., about 5% of our baseline prediction.
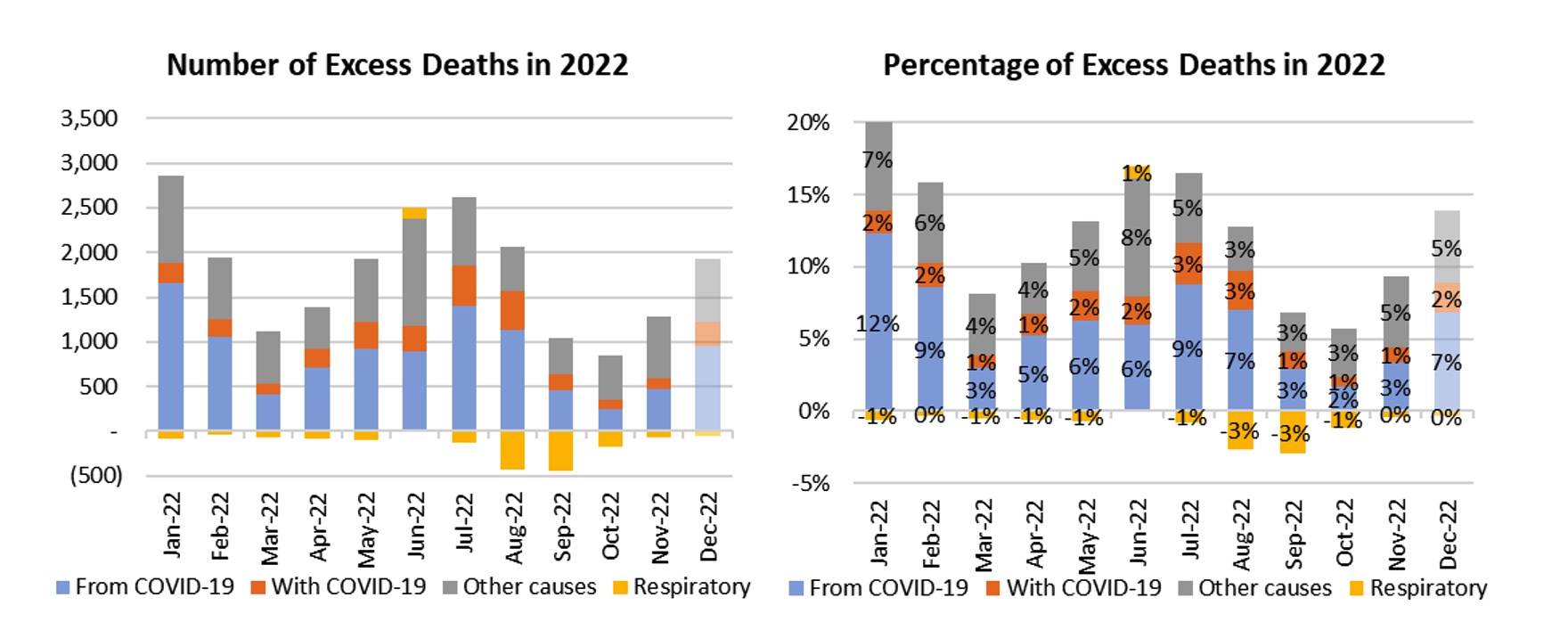
This estimation process results in total excess deaths for the month of December of 14% of predicted, half of which (7% of predicted) are from COVID-19 and another 15% (2% of predicted) are with COVID-19.
For the whole of 2022, our estimate is that excess deaths were 12%. In other words, there were nearly 20,000 more deaths in 2022 than would have been expected if the pandemic had not happened. Of these, 10,300 were from COVID-19, with another 2,900 with COVID-19. The remaining 6,600 excess deaths were from other causes, with 1,500 fewer deaths than expected from respiratory causes and 8,100 excess deaths from other non-COVID-19 causes.
Figure 7 – Excess deaths per month in 2022 (including estimate for December) *
Excess deaths to 30 November by Age/Gender
Table 2 below shows our estimate of excess deaths by age band and gender. We have shown the excess including all deaths, and then again after deducting from and with COVID-19 deaths.
Table 2 – Excess deaths in Australia – By Age/Gender*
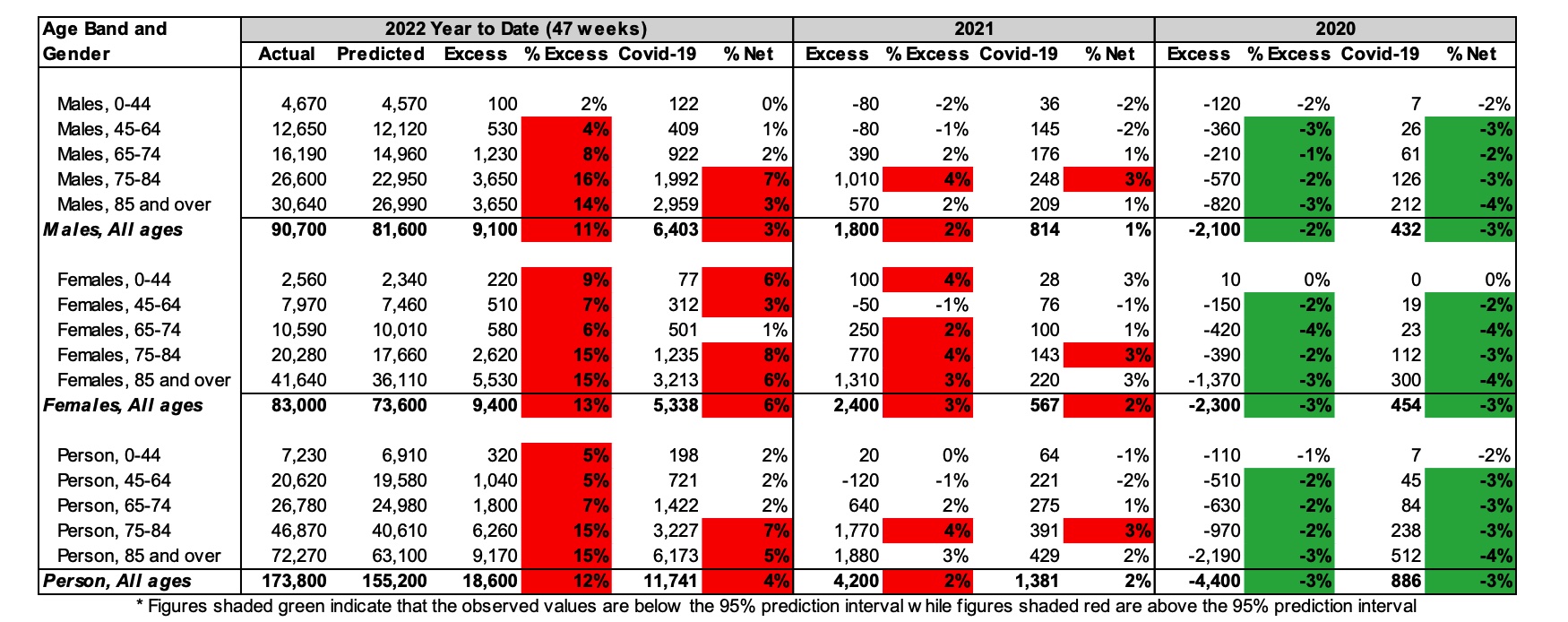
* COVID-19 data from ABS customised report 2023
Almost all age bands show excess deaths in 2022 (which is not all that surprising given the excess deaths for the whole population), but the number and percentage of excess deaths is higher in older age bands. The risk of mortality from COVID-19 is steeper than the underlying age mortality curve, so this result is somewhat expected.
However, it is notable that there are excess deaths in all age groups and that this excess is generally significant, even after removing COVID-19 deaths. To look at this further, we have shown these results similarly to the graphs by cause, showing weekly excess deaths by age band since the start of the pandemic. For these charts, we have been able to show the contribution of deaths from and with COVID-19 (in orange) separately to non-COVID-19 deaths. The 95% prediction interval is also shown. All age bands are shown using the same y-axis to give a sense of contribution of each age band.
Figure 8 – Weekly excess deaths in 2020-22 by age band (all persons)*
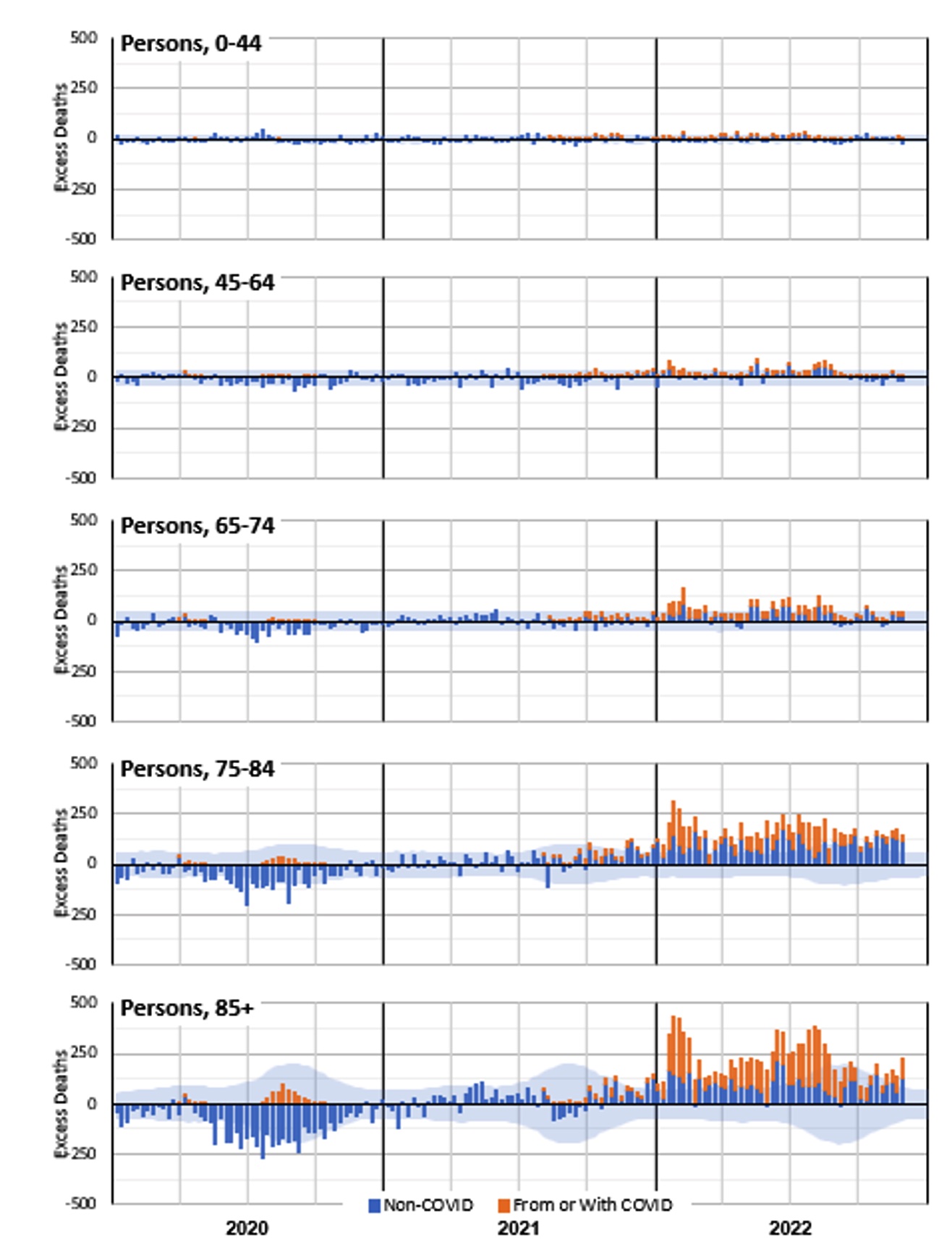
* COVID-19 data from ABS customised report 2023
Figure 8 shows that excess deaths in 2022 are dominated by the older age groups. However, we already expect many more deaths in these age groups. It is instructive to consider the same information with the excess deaths expressed as a percentage of predicted deaths.
Figure 9 – Weekly excess deaths as a % of predicted in 2020-22 by age band (all persons)*
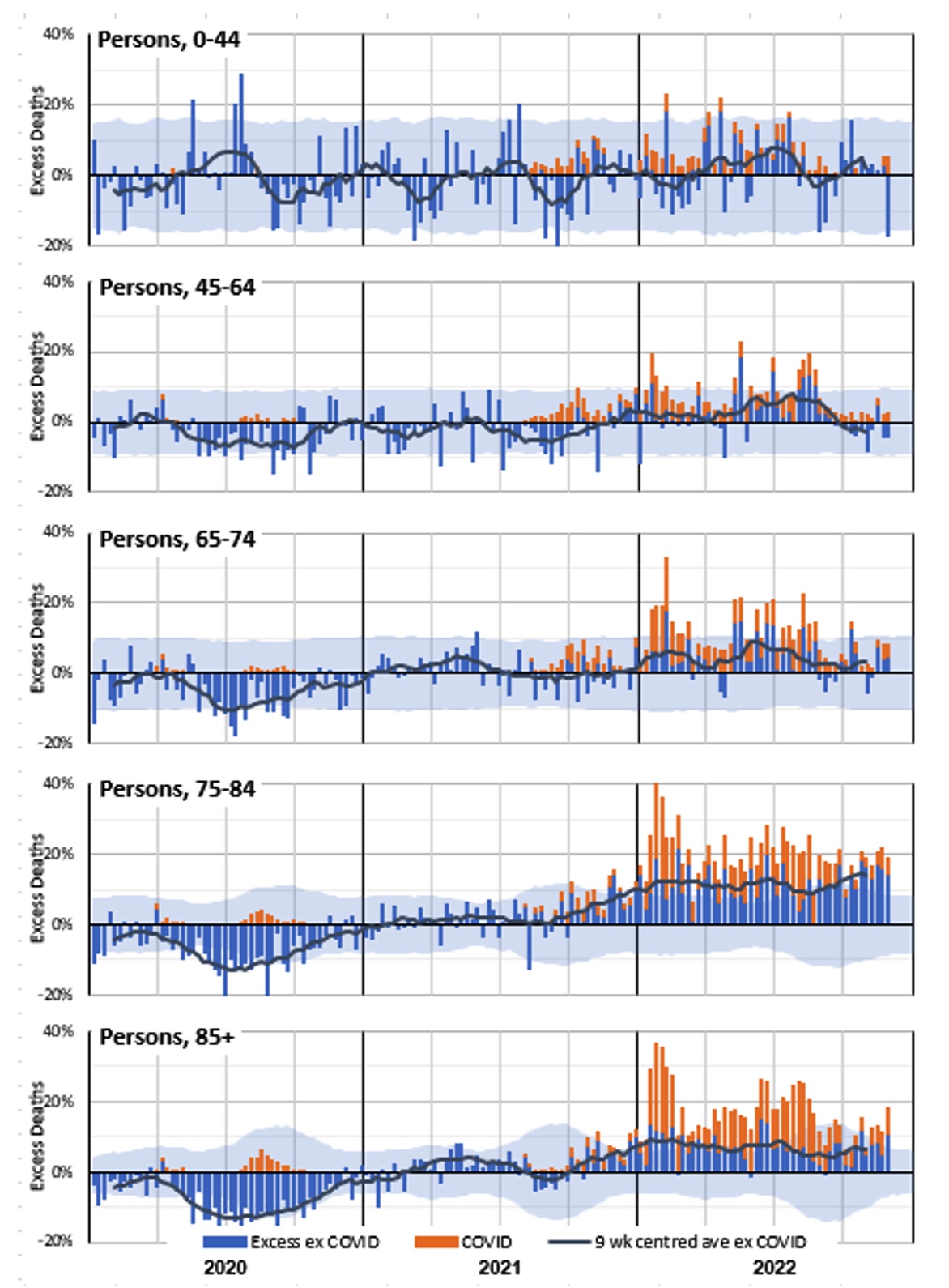
* COVID-19 data from ABS customised report 2023
Figure 9 shows that the older age groups still experienced the most significant increase in excess deaths when expressed as a percentage of predicted deaths. Indeed, deaths of people over the age of 75 are significantly higher than expected in almost every week of 2022.
While the numbers of deaths in the 0-44 and 45-64 age bands are small, we saw in Table 2 that year-to-date excess deaths in 2022 are materially higher than expected. That table also showed that the percentage excess was higher for females than for males. The differences are worth investigation, although the small numbers mean that there is considerable natural variation.
Figure 10 – Weekly excess deaths as a % of predicted in 2020-22 for ages 0-44 and 45-64 by gender*
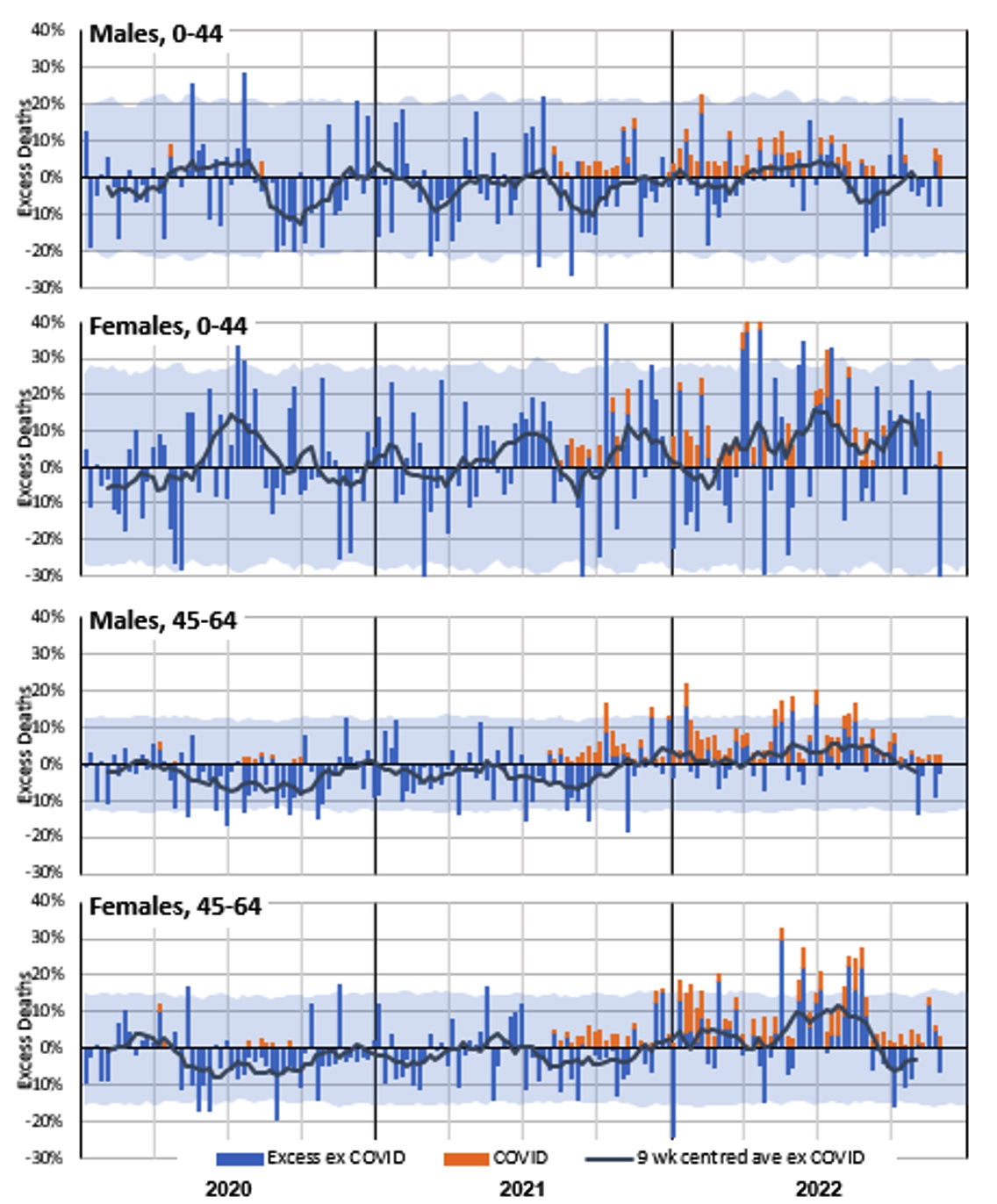
* COVID-19 data from ABS customised report 2023
Figure 10 shows that female non-COVID-19 mortality experience in 2021 and 2022 is noticeably worse than male, especially in the 0-44 age band.
Excess deaths to 30 November 2022 by State/Territory
Table 3 shows our estimate of excess deaths by state/territory, before and after deducting deaths from and with COVID-19. Data is grouped for smaller states/territories, where small numbers meant that the ABS could not give us detailed COVID-19 figures.
Table 3 – Excess deaths in Australia – By State/Territory for 2022 to 27 November (47 weeks)*
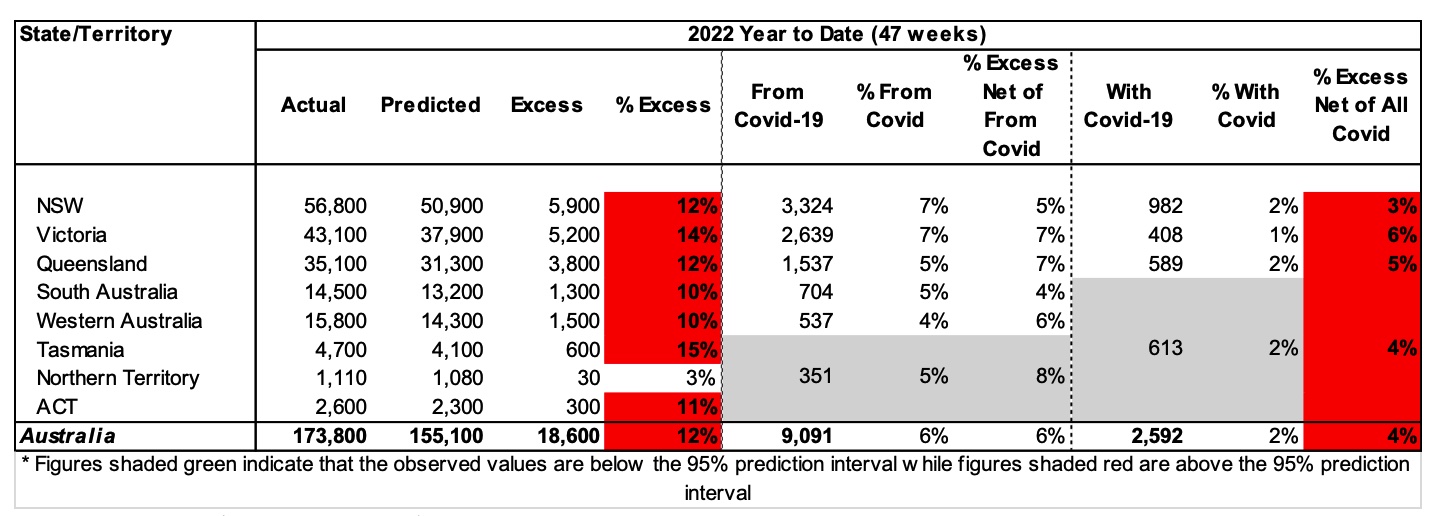
* COVID-19 data from ABS customised report 2023
In 2022, all states/territories apart from NT had significant levels of excess mortality ranging from 10% to 15% of predicted. Generally, about half of this is due to deaths from COVID-19, with another 1-2% due to deaths with COVID-19.
The graphs below show these results week-by-week (with the excess shown as a percentage of the predicted value) for:
- the three largest states (NSW, Victoria and Queensland) where we have weekly information on both from and with COVID-19 deaths;
- SA and WA where we have weekly information on deaths from COVID-19 only; and
- the smaller states/territories (Tasmania, NT and ACT) where weekly information on COVID-19 deaths is not available.
Figure 11 – Weekly excess deaths as a % of predicted in 2020-22 for NSW, Victoria, Queensland*
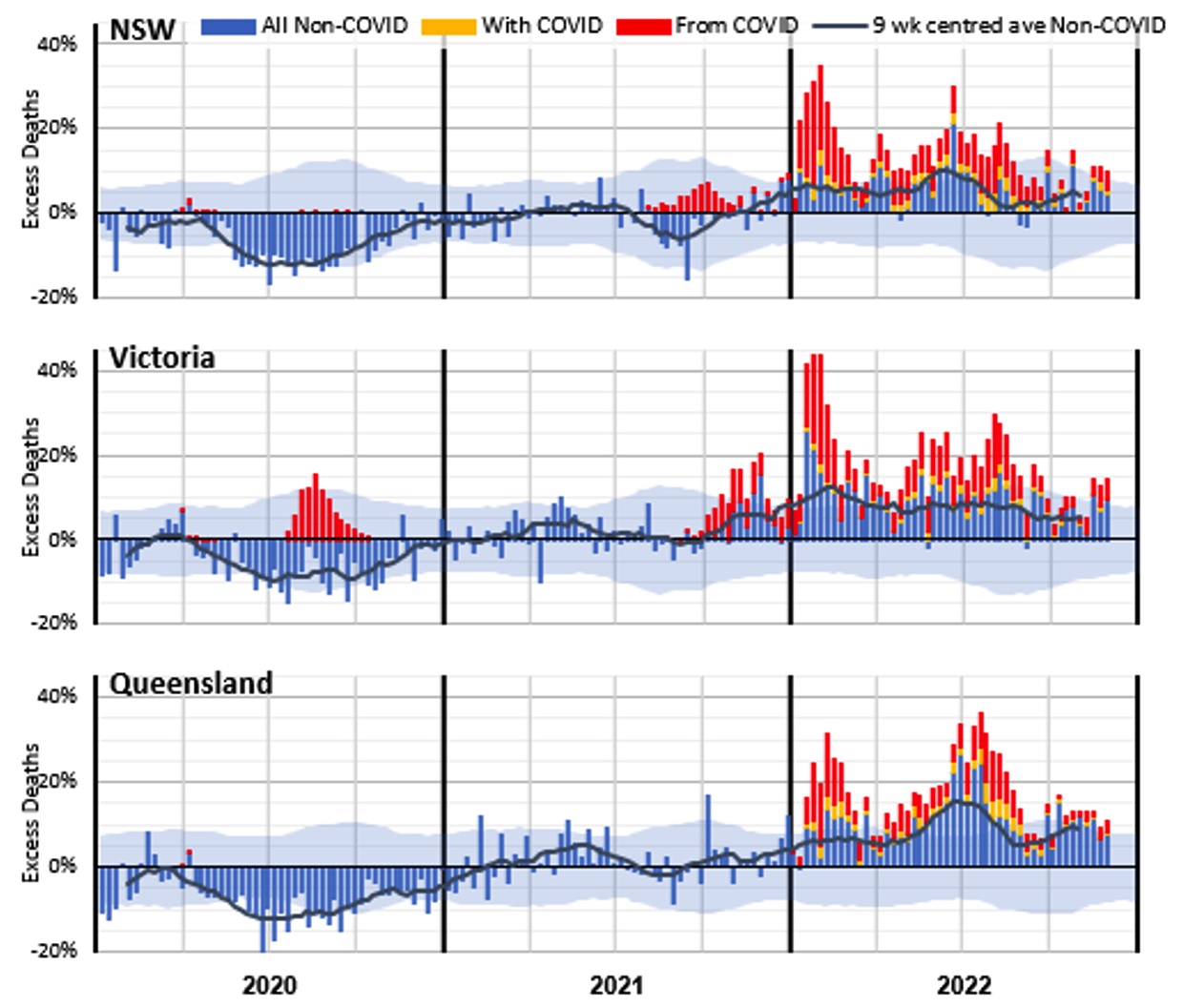
* COVID-19 data from ABS customised report 2023
Figure 11 shows that these larger states all had better-than-expected mortality in 2020. It also shows the impact of the second COVID-19 wave in Victoria.
In 2021, Victoria shows a much higher level of excess deaths in the Delta wave – in the last quarter of the year – than either NSW or Queensland. A large portion of these deaths do not have COVID-19 on the death certificate.
In 2022:
- Queensland had a large peak in non-COVID excess deaths in the middle of the year (at the time of flu and COVID-19 waves). NSW had a smaller peak at this time, but Victoria did not have a similar peak; and
- barring the winter peaks for NSW and Queensland, Victoria’s non-COVID-19 excess has tended to be higher than the other two large states.
Figure 12 – Weekly excess deaths as a % of predicted in 2020-22 for WA and SA*
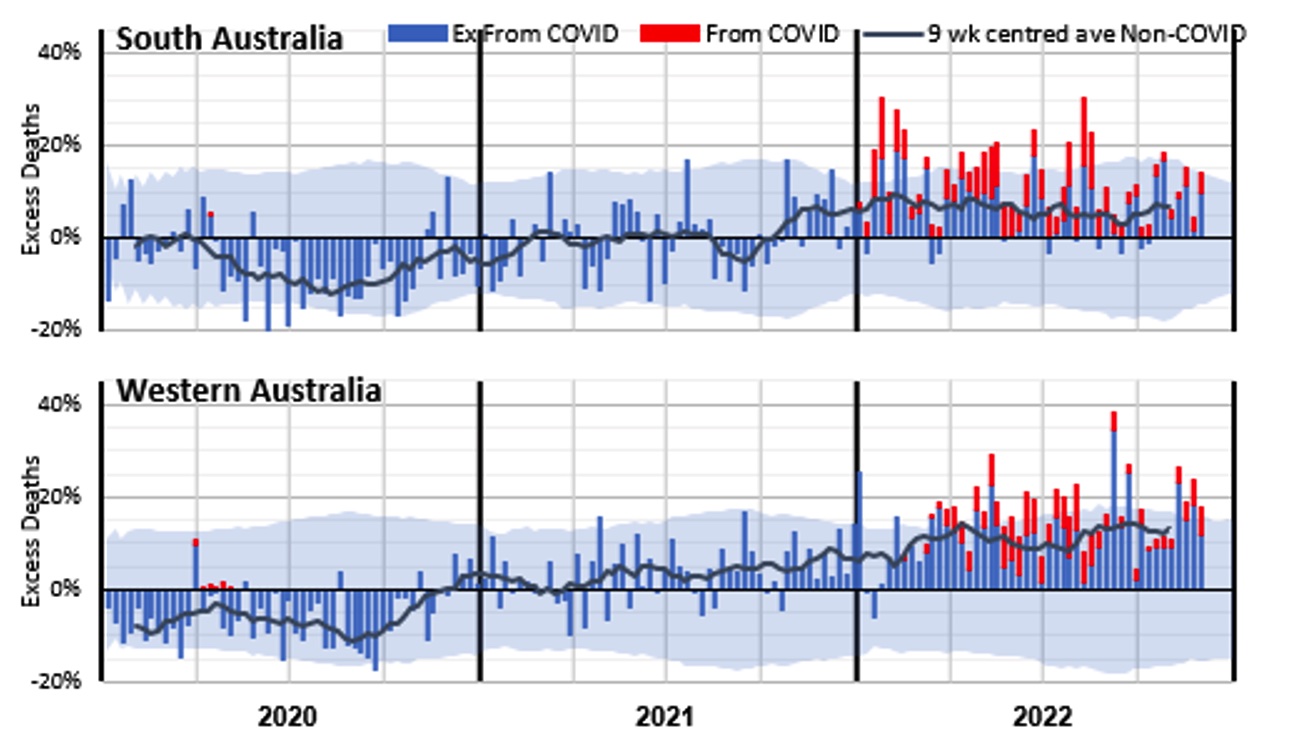
* COVID-19 data from ABS customised report 2023
The SA experience is similar to the three largest states, although somewhat more volatile given its smaller size.
Western Australia, while mostly having excess deaths within the 95% prediction interval, had many more weeks with positive excess deaths than with negative excess deaths. There is no large COVID-19 spike in January/February, thanks to the later opening of WA’s borders.
Figure 13 – Weekly excess deaths as a % of predicted in 2020-22 for Tasmania, ACT and NT
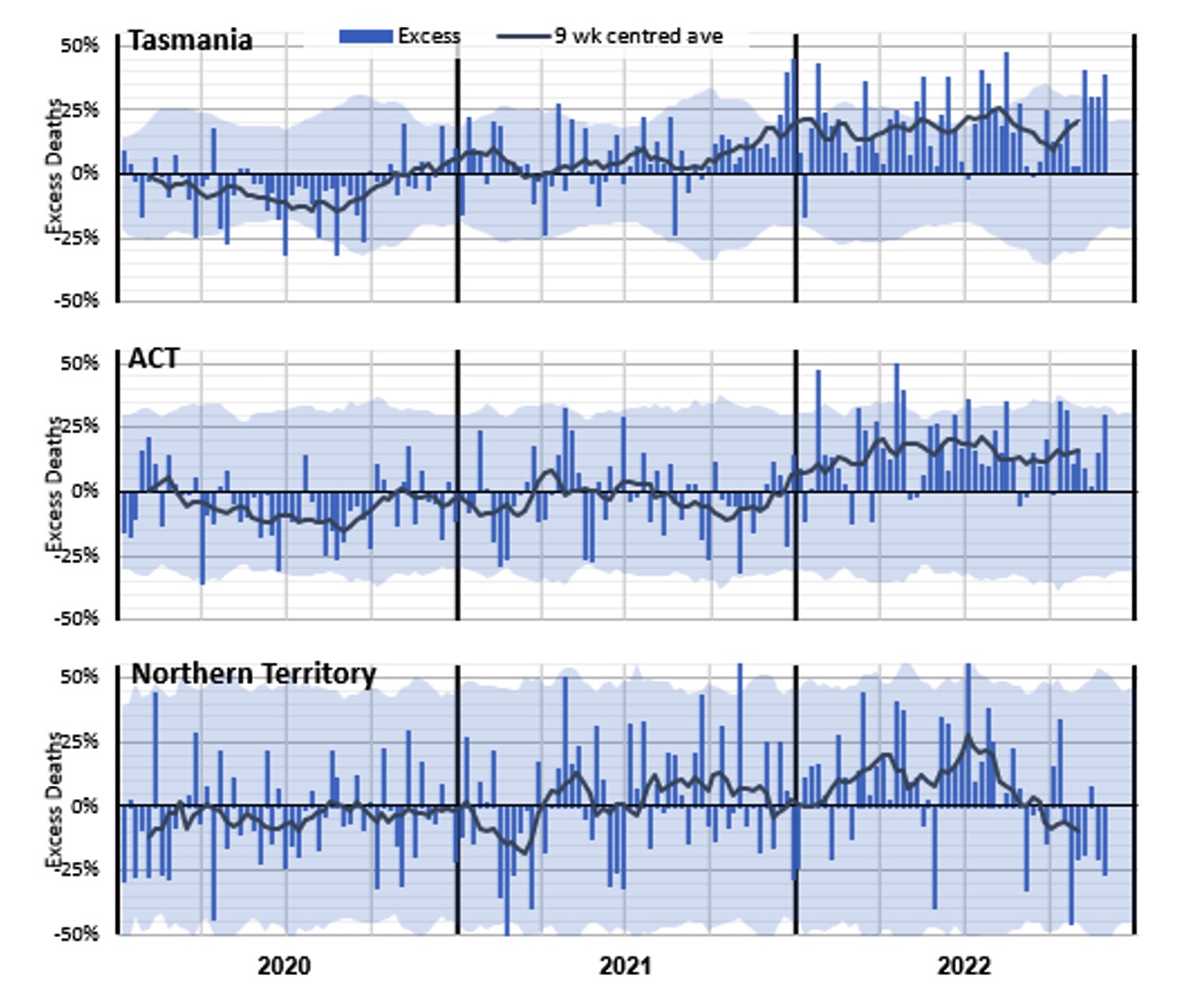
Figure 13 shows the higher volatility of excess mortality experienced by the smallest state and the two territories. Allowing for that volatility, Tasmania had broadly the same experience of excess mortality as the larger states, but with a high level of excess deaths during the Delta wave late in 2021.
With its relatively young and affluent population, the ACT has experienced lower excess mortality than the larger states.
The Northern Territory has a very young population, which might explain the low net impact of the pandemic after allowing for the high volatility caused by a very small weekly expected death count. There is no apparent general trend in excess mortality, although it does appear to have been declining since the middle of 2022.
What could be causing the non-COVID-19 excess deaths?
The measurement of higher numbers of deaths than predicted does not tell us why this is occurring. There are several reasons hypothesised around the world (where this effect is occurring to a greater or lesser extent). It isn’t possible to identify from death counts alone what is causing the non-COVID-19 excess deaths, but we have listed below the most likely explanations. We note that multiple factors are likely in play, and different factors may be more or less pronounced at various times.
To summarise the evidence from earlier sections:
- deaths with COVID-19 have followed the same pattern as deaths from COVID-19 in 2022;
- non-COVID-19 excess deaths have been highest when there have been peaks in COVID-19 deaths and peaks in influenza deaths;
- deaths due to some causes (dementia and “other” diseases in particular) are closely correlated to the level of respiratory disease (including COVID-19) circulating;
- non-COVID-19 excess deaths are particularly apparent in the oldest two age groups for both genders, and the youngest two age groups for females only;
- non-COVID-19 excess deaths are less apparent when there is no or little COVID-19 circulating, as illustrated by the difference between WA and the other states in early 2022.
Based on these observations, the following indicates which factors, in our view, are likely to be having a greater or lesser impact on Australian excess mortality in 2022.
- Post-COVID-19 sequelae or interactions with other causes of death: Studies have shown that COVID-19 is associated with higher subsequent mortality risk from heart disease and other causes, but certifying doctors would generally not identify a causative link several months after recovery from COVID-19. Therefore, it seems likely that there would be more of these deaths than identified. The age-based analysis supports this hypothesis, with non-COVID-19 excess deaths occurring in 2022 even in those under 45, noting that this age group has had low levels of COVID-19 deaths. The absence of excess deaths in WA in January also supports this explanation. Likely impact in Australia: High.
- Delay in emergency care: Pressure on the health, hospital and aged care systems, including ambulance ramping and bed block, could lead to people not getting the care they require, either as they avoid seeking help, or their care is not as timely as it might have been in pre-pandemic times. The peaks in non-COVID-19 excess deaths at times of high COVID-19 and/or influenza deaths supports this hypothesis. Likely impact in Australia: High during COVID-19 and influenza peaks.
- Mortality displacement: Australia had negative mortality displacement (i.e. fewer deaths than expected) in the first year or so of the pandemic, resulting from the absence of many respiratory diseases. The lower-than-expected mortality from respiratory disease was again apparent in 2021. As such, some of the excess we have seen in some causes in 2021 and 2022 may be the reversing of this effect. People who otherwise may have died earlier had their systems been stressed by respiratory disease may now be succumbing to their underlying illnesses. Conversely, the earlier-than-usual flu season in 2022 appears to have resulted in some forward mortality displacement. Likely impact in Australia: Moderate, likely to reduce over time.
- Delay in routine care: Opportunities to diagnose or treat non-COVID-19 diseases have been missed for various reasons including fear and lack of opportunity. There is some evidence that this may be affecting cancer deaths. It may also be a factor in higher deaths from other causes, such as ischaemic heart disease, diabetes, and the large “other” category. Likely impact in Australia: Low to Moderate, likely to increase over time.
- Undiagnosed COVID-19: Some of the excess deaths could be from unidentified COVID-19. This effect happened early in the pandemic, but it seems less likely in 2022, as testing is much more available, particularly for those who are seriously ill (although for mild illness, testing is clearly reduced). While for any deaths where COVID-19 may be suspected, post-mortem testing is occurring in Australia, it is possible that some deaths caused by COVID-19 with unusual symptoms (e.g. some sudden cardiovascular deaths) may not be identified as caused by COVID-19. The timing of the higher levels of non-COVID-19 excess deaths (once deaths with COVID-19 are also removed) coinciding with high levels of COVID-19 deaths suggests that there may be some undiagnosed COVID-19 deaths. Likely impact in Australia: Low, perhaps higher during COVID-19 peaks.
- Mental health issues: There has been much discussion throughout the pandemic about the impacts on mental health, including commentary that lockdowns and other measures are causing an increase in suicide deaths. Data from the latest ABS Causes of Death, Australia publication shows that age-standardised suicide rates for both males and females were lower in 2020 and 2021 compared with the preceding three years, noting that the 2020 and 2021 data is preliminary. The publication also shows that 3.2% of suicide deaths in 2020 (0.06% of all deaths) and 2.6% in 2021 (0.05% of all deaths) had the pandemic mentioned as a risk factor. Even where the pandemic was a risk factor, there were, on average, five other risk factors. The suicide monitoring reports for NSW and Victoria show the same picture for 2020 and 2021, with 2022 slightly higher in NSW and Victoria, but a very small proportion of all deaths. (Lifeline: 13 11 14) Likely impact in Australia: Low.
- Pandemic-influenced lifestyle changes: There is evidence from the UK that a higher proportion of people made less healthy lifestyle choices during lockdowns (e.g. drinking more alcohol, exercising less, higher rates of childhood obesity), and that these less healthy practices have continued. It is unclear to what extent similar factors may be affecting mortality in Australia in 2022. Deaths directly caused by drug and/or alcohol abuse are relatively low, compared with those from other causes, but there would be an indirect impact. Likely impact in Australia: Low.
- Vaccine-related deaths: While there have been deaths in Australia caused by the administration of COVID-19 vaccines, the number of such deaths has been small. Australia has a very good vaccine approval and safety monitoring processes, administered by the Therapeutic Goods Administration. The latest vaccine safety report (to 23 February) shows that, of the 976 reports of death following vaccination, only 14 were found to have been caused by the administration of the vaccine. The TGA makes it clear that the remaining 962 were not caused by COVID-19 vaccination. That is, they were due to other, unrelated causes. In addition, the vaccine rollout ramped up slowly from February 2021, with high rates of vaccination in August to October 2021 and again in January 2022, but has been low for most of 2022. This does not fit with the timing or shape of the excess mortality. Likely impact in Australia: Negligible.
Figure 14, which shows excess deaths from doctor-certified respiratory disease, other non-COVID causes and those from COVID-19, puts the above into context, across the pandemic. Note that deaths with COVID-19 are included with the primary non-COVID cause (respiratory or other).
Figure 14 – Possible causes of non-COVID-19 excess mortality from time to time during the pandemic*
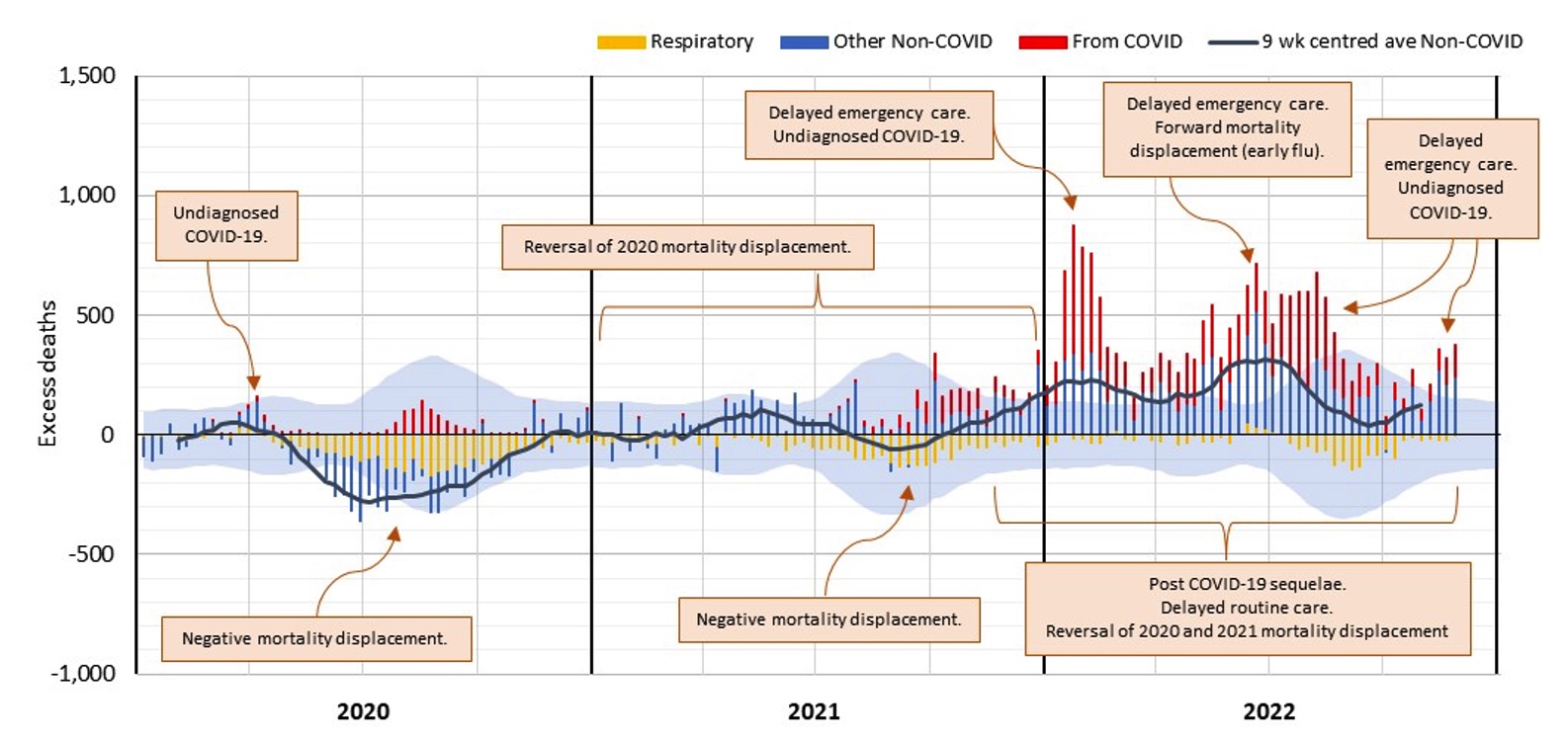
* COVID-19 data from ABS customised report 2023
Standardised Mortality Rates
Figure 15 shows the cumulative standardised mortality rates (SDRs) for 2015 to 2022, expressed relative to the rate for 2019. The SDRs are from the Provisional Mortality Statistics, plus allowance for late-reported deaths.
Figure 15 – Cumulative standardised mortality rate relative to 2019
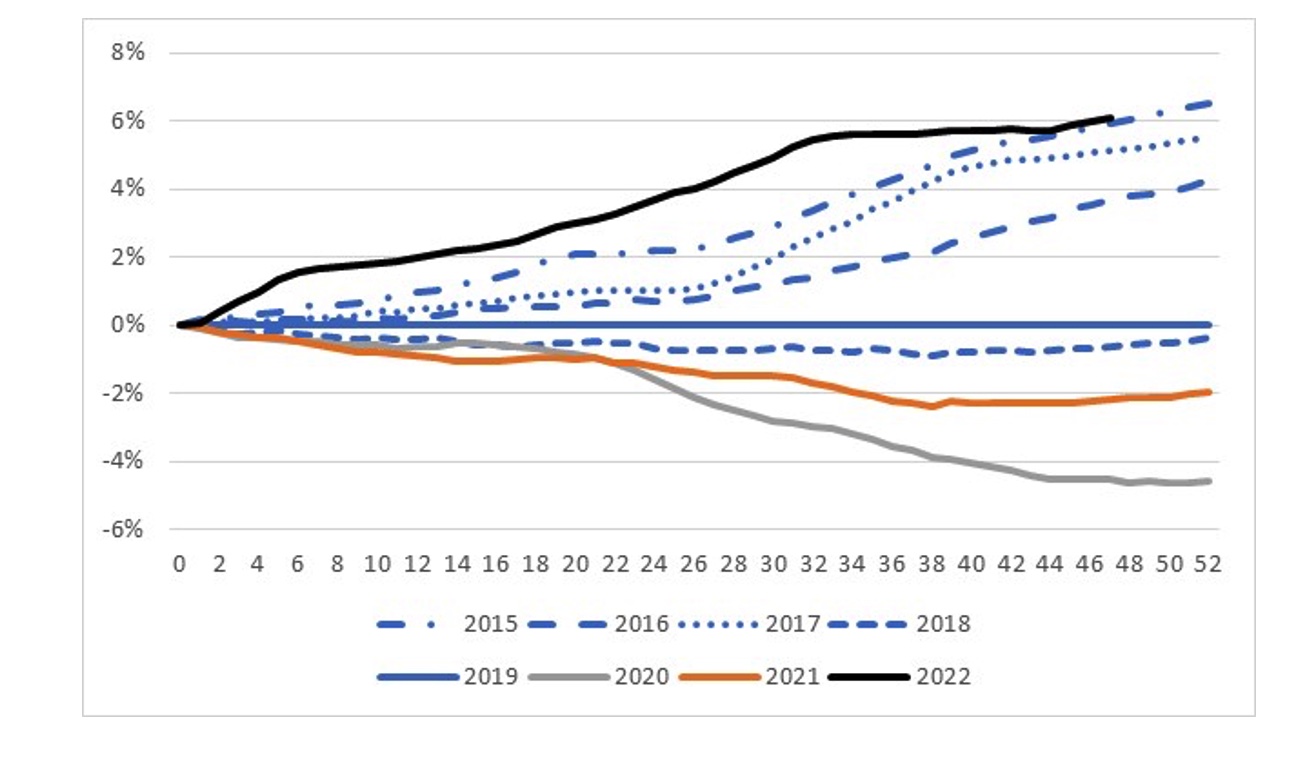
The graph shows that:
- Mortality rates improved over the 2015 to 2019 pre-pandemic years, noting that both 2017 and 2019 were “bad” influenza years, resulting in higher than usual deaths both from and related to influenza;
- the 2020 year is considerably lower than 2019, a result of the lower number of respiratory and respiratory-related deaths in that year due to measures introduced to curb COVID-19;
- 2021 is higher than 2020, a combination of both deaths from COVID-19 during the Delta wave and excess mortality from other causes of death; and
- for 2022, after being well above all other years shown for much of the year, experience in the last few months has now almost converged with the 2015 year, sitting around 6% higher than 2019.
A mystery partly solved?
One question that regularly crops up is why COVID-19 deaths reported by Victorian health authorities appear to be so much higher than those reported by NSW. The customised data that we have received from the ABS allows us to shed a little light on this, although some questions still remain.
The customised data that we have received from the ABS includes deaths both from and with COVID-19 for each of NSW and Victoria for 2022, with the deaths summarised into the week that they occurred.
From the Federal Department of Health website we also have 7-day averages of the surveillance deaths reported by each state/territory health authority, summarised by the date the death occurred. The 7-day averages are reported in whole numbers only, but by multiplying by 7 we get an approximate number of surveillance deaths reported for each week of occurrence.
Per the national surveillance definition, deaths are reported as COVID-19 deaths if a person died with COVID-19, not necessarily because COVID-19 was the cause of death. Deaths are only excluded if there is a clear alternative cause of death that is unrelated to COVID-19 (e.g. trauma). As such, surveillance deaths will include deaths from COVID-19, deaths with COVID-19 and other deaths where the doctor/coroner has determined that COVID-19 was incidental and had no role in the death of the person.
By comparing the two datasets, we can estimate the number of surveillance deaths reported that do not end up with COVID-19 recorded on the death certificate.
Figure 16 shows, for each of NSW and Victoria, surveillance deaths expressed as a percentage of predicted deaths, broken down into those from COVID-19, those with COVID-19 and those where COVID-19 does not appear on the death certificate.
Figure 16 – Surveillance deaths as a % of predicted deaths
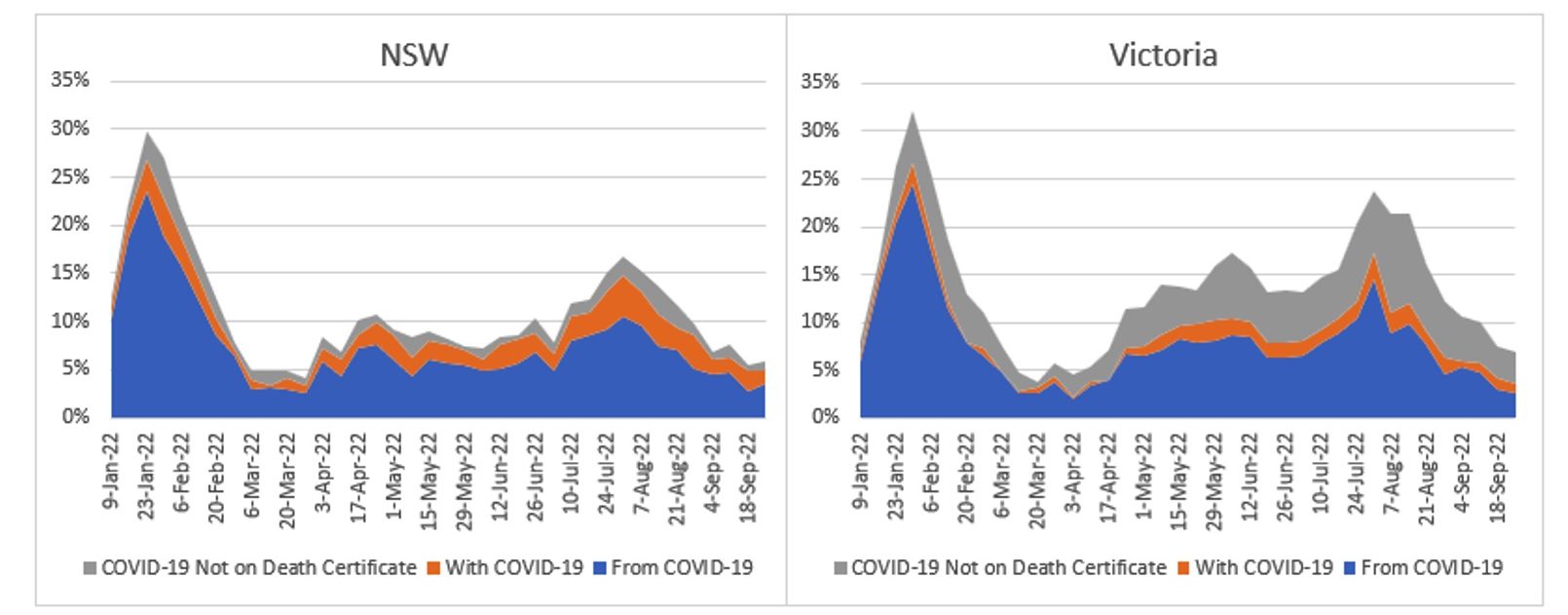
* From and With COVID-19 data from ABS customised report 2023
We can see that:
- deaths from COVID-19 are very similar for the two states, as a proportion of predicted deaths;
- Victoria has slightly lower deaths with COVID-19; and
- Victoria has significantly more surveillance-reported deaths that do not eventuate to have COVID-19 coded on the death certificate.
We do not have an explanation for why Victoria would record more surveillance deaths than NSW.
Disclaimer
This monthly COVID-19 mortality analysis is intended for discussion purposes only and does not constitute consulting advice on which to base decisions. We are not medical professionals, public health specialists or epidemiologists.
To the extent permitted by law, all users of the monthly analysis hereby release and indemnify The Institute of Actuaries of Australia and associated parties from all present and future liabilities that may arise in connection with this monthly analysis, its publication or any communication, discussion or work relating to or derived from the contents of this monthly analysis.
COVID-19 Mortality Working Group
The members of the Working Group are:
- Angelo Andrew
- Karen Cutter
- Jennifer Lang
- Han Li
- Richard Lyon
- Zhan Wang
- Mengyi Xu
CPD: Actuaries Institute Members can claim two CPD points for every hour of reading articles on Actuaries Digital.




